A client ends a strong session and says, “Can I add you on Instagram?” or “Do you want to grab coffee sometime?” In the moment, it can feel like a quick, harmless yes, especially if you want to support rapport or you sense the client might feel rejected.
That said, that one yes can create instant complexity: what you do if they message at 11 p.m., comment on your family photos, or expect faster replies than your usual turnaround. Boundary issues are a leading driver of complaints and poor outcomes, and unclear boundaries can increase dropout risk by around 20%, because the client may feel confused about what the relationship is and what care they can count on.
By the end of this section, you’ll be able to name the core boundary domains and use a repeatable way to respond in real time without sounding cold. Think of boundaries as what stays consistent even when the client’s needs, risk level, or attachment pull changes.
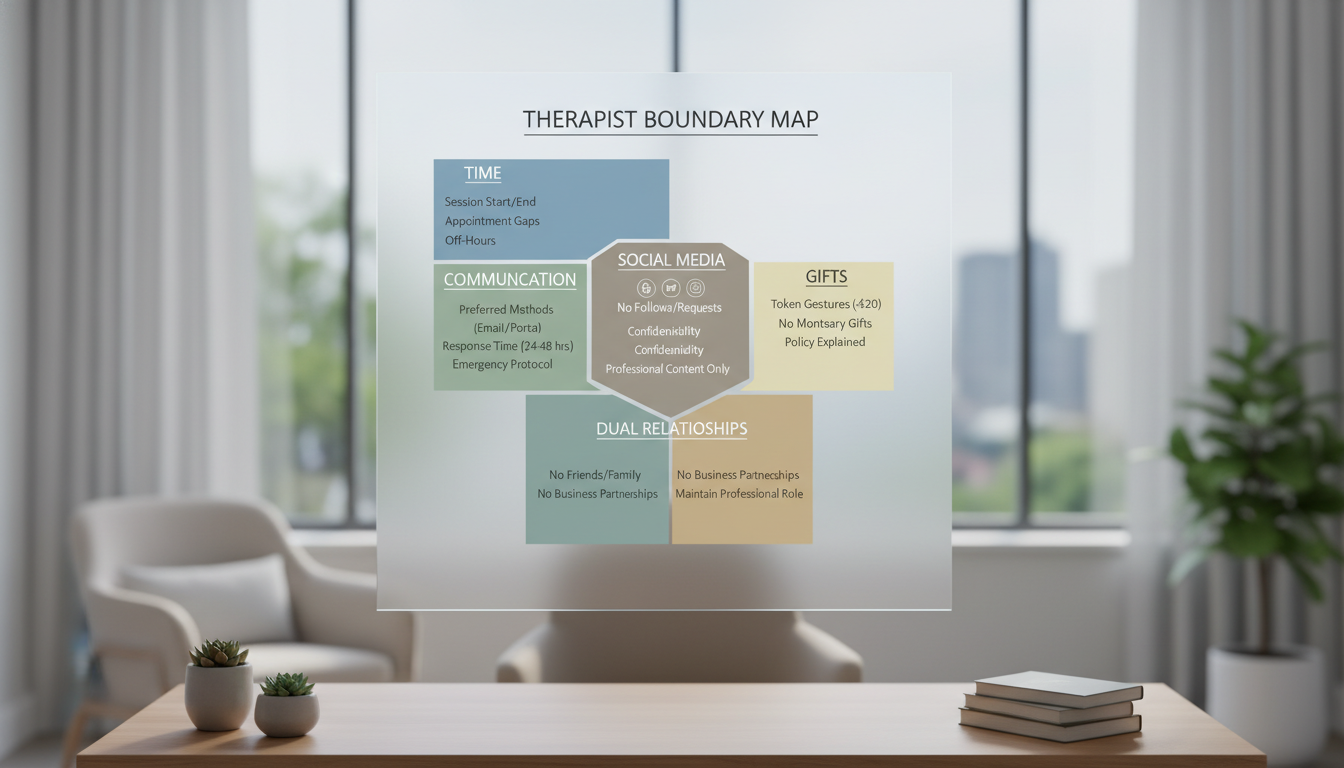
Core boundary domains to keep clear (so you can respond quickly):
Communication: where messages go, response times, and what counts as urgent
Time: session length, late cancellations, and after-hours contact
Place: meeting locations and what is and is not a therapy setting
Money: fees, billing questions, and payment exceptions
Roles: therapist vs friend, mentor, advocate, or business contact
Privacy: social media contact, online visibility, and what you share about yourself
If you do one thing, do this: pause before answering and name the domain out loud. For example, “I hear you want to stay connected between sessions. Let’s talk about what support looks like between appointments and the best way to reach me.”
Common mistake: explaining too much or apologizing until it sounds negotiable. Fix: keep it warm, brief, and specific, then offer an approved alternative (for example, secure messaging during set hours, a check-in slot, or a crisis line for emergencies). Works best when you state the boundary early and consistently; it tends to fail when you make exceptions in the first 2 to 4 weeks, because the client learns a different rule than the one you plan to follow.